

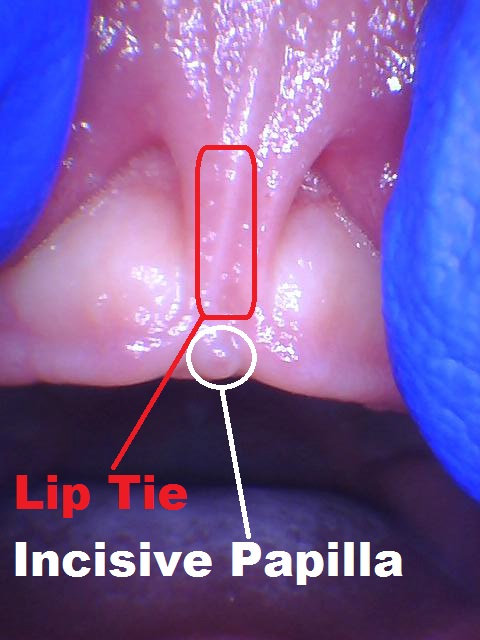
55 Reasons Parents Choose to Release Their Infants Lip Ties
BREASTFEEDING: During proper breastfeeding or bottle feeding, infantile suckling demands the lips be a major contributor of an adequate seal for vacuum generation. This vacuum generation requires a 100% seal around breast tissue or bottle nipple. If this seal is 99% or less due to potentially a variety of factors including a lip tie then air intake may ensue. This air intake has many associated negative effects on the infant including pain due to excess eating of air pressing against the gastrointestinal system and surrounding tissues of the abdomen. Air is not nutritious and this lack of calories leads to frequent hunger pains, leading to necessity of frequent feedings that may account for loss of body weight and sleep deprivation for both the infant and the parents. You can imagine the medical urgency of infant weight loss as well as the psychological consequences of sleep deprivation for the parents. Most babies react to this feeding crisis by deviating away from optimum infantile suckling mechanism; even though such compensation is better than giving up, it may lead to a host of other problems. By having to perform this physical suckling task incorrectly some babies develop muscular imbalances; muscular imbalances may be defined as the "wrong muscles getting stronger, and the right muscles getting weaker". The longer that compensation is left unattended the higher the chance muscular imbalances become more pronounced, time needed to unwind from it may increase, and the number of sessions of physical therapy/bodywork needed to rebalance muscles and nerves may rise. With regards to "the latch quality" there may be some tell tale signs from the outside appearance of breastfeeding or bottle feeding; so an educated professional can do some visual constructive assessment by direct observation to be sure; however, since each child's and each mother's anatomy is different, plus the technique, milk supply and host of other factors may differ, it is useful to include other subjective and objective functional signs as red flags that something may be "wrong"; a few of which I have itemized below, none of which require direct viewing of the breastfeeding mechanism:
Discomfort Due to Hunger poor latch may lead to less food intake
Frequent feedings inefficiency exhaustion and filling up with air
Long feeding times poor seal leads to poor suction to poor intake
Weight Loss of infant poor intake amount and overworking baby
Supplemental feedings bottles w/pumped, formula, or donated breast milk
Loss of sleep of infant due to hunger and constant feeding
Loss of sleep of parent due to constant feeding and infant cry
Pain to mother due to infant biting/clamping/compression of nipples
Mastitis damage to milk ducts by poor drainage of mother's breasts
Bleeding nipples by biting baby who cannot suckle correctly
Infection of breast tissue secondary to skin damage by biting baby
Reduction of mother's breast milk supply due to low drainage, pain
COLIC: An infant's physical reactions to sustained discomfort of bloating are traditionally described as "colic". Colicky baby's physical manifestations include prolonged raised or pulling in of limbs, clenched fists, arching of back, tight bloated tummy, passing of much gas, and generally an unhappy baby.
Bloating due to excess air intake in the gastrointestinal system
Bodily Tension stiff limbs, clenched fists, arched back, tense abdomen
Unhappy Baby prolonged and intense crying for no apparent reason
ORTHODONTICS: A lip tie is a major contributor to a gap between the front teeth. It is imperative to note that dental spacing is multi-factorial: jaw size, tooth size, functional habits also play key roles here. Nevertheless, lip ties do try to create a gap between the front teeth, and a lip tie release procedure can be a very effective treatment option.






A lip tie may not succeed in creating a space based on the sum of the said multitude of forces at play. But, if there is a gap between the front teeth, aka diastema, then the patient may be more inclined to spend the next significant number of years and monies correcting the problem with orthodontics; and then still proceed to have the frenectomy done post-braces as retention to minimize the possibility of the gap reopening.




As you can see above, closure of dental gap with braces does NOT remove the lip tie; not only the soft tissue problem still exists, but it may reopen the space within hours. Your orthodontist will help you plan for retention of this closure, whether it includes a tie release or not; for those not comfortable with a lip tie release please consider a permanent retainer to help you maintain the orthodontic results you have achieved.
Orthodontic care, whether fixed metal braces or removable plastic Invisalign, may cost a patient more than time and money. Plaque is a major component of tooth decay and orthodontic appliances are major plaque traps that pose an increased risk of tooth decay during orthodontic treatment. Head gear and braces were an extremely constructive component of my own growth and development; enough to inspire me to take up the dental profession; however, minimizing the need or the duration of orthodontic service is what is being examined here.
Time spent in orthodontic care to close gap
Financial cost of orthodontic care to close gap
Damage to permanent teeth possible during orthodontics
Gap can re-open requiring frenectomy or more orthodontics
SPEECH: With regards to whether dental spacing can affect speech, the answer is yes. In my experience the space does not usually cause speech problems, but it certainly can and it does. Some people will compensate fine for the space without an audible issue while others are spitting while they talk...right out of the mouth and onto another's eye. It may be offensive or alarming for the eye owner. It may be embarrassing for the mouth owner. Food, liquid, and sound may escape this "space" during functions of eating and talking as pressure is built up in the oral cavity. Others go out of their way not to allow such potentially embarrassing effects and consistently close their dental gap with their tongue during function. The result of such consistent gap closure by the tongue may become habitual also known as tongue thrust, frequently a hard habit to break. A sign of tongue thrust may be altered speech where the tongue is postured differently as it shoulders the extra burden of gap closure while talking.
Spitting while talking as gap undermines seal
Tongue thrust as compensation alters tongue posture
Speech altered as tongue manages saliva, sound, and gap
EATING SOLIDS: the tongue is a major component of proper swallowing mechanism; hence the role of tongue ties as a potential contributor of feeding problems self-evident. However, lip ties can influence the eating mechanism of solids as well. There is a band of tissue, an attached layer of gingiva next to the teeth called the keratinized layer, also commonly referred to as the "gums". It is a much stronger layer of oral tissue that is meant to withstand the forces of mastication and various textures of food. As individuals we are blessed with different amounts of this keratinized layer of gum tissue or what I refer to as armored tissue.


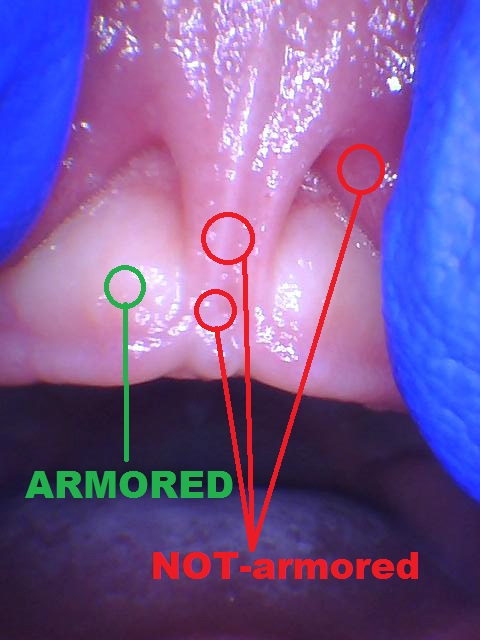
Lip ties as well as non-restrictive lip frenums are covered by a layer of non-armored tissue that may lay close to the teeth(gumline); if this non-armored weak tissue is indeed close to the gumline it can pose a problem while biting into food. During mastication, solids rub against the lip tie or lip frenum and may cause discomfort that alters feeding behavior prompting statements such as "oh no, I like apples....I just don't like to bite into them". In the case of the toddler they are seen as shying away from solids and are later labeled as picky eaters. This may translate into poor nutrition as care givers may eventually become exhausted with workarounds.
Pain with biting into solids
Poor nutrition picky eater
Eating altered as tongue manages liquids, solids, and gap
ORAL HYGIENE: Lip ties can pose a challenge to proper brushing of teeth. The keratinized or armored layer next to teeth can easily tolerate the bristles of a soft toothbrush, as well as better resist the toxins of nearby dental plaque. The non-armored oral tissue that covers the lip tie and lip frenums may become a source of aggravation when brushed by toothbrush bristles. Despite all the preparation, on baby's first day of tooth brushing, a parent's best wishes of good oral hygiene is deflated when their toddler abruptly and consistently turns his/her head to avoid such contact with Mr. Toothbrush. Seasoned parents and dental professionals alike are sometimes puzzled over why a normally cooperative and coordinated adolescent has plaque buildup on the front teeth where normally that area is exceptionally easy to keep clean.




Please be advised that I have observed many children who are not at all bothered by the toothbrush bristles rub of their lip ties, while others go on to become aggravated. In due time, the plaque buildup will most likely promote gingivits; and in some individuals, the unattended dental plaque wears down the tooth enamel and becomes associated with dental caries and many other not so wonderful things my beloved field of dentistry is famous for.
Pain with tooth brushing
Plaque accumulation
Bad breath due to dental plaque
Gingivitis due to dental plaque
Cavities due to dental plaque
Class time lost to restorative dentistry
Money lost to restorative dentistry
Pain with restorative dentistry
Food clearing reduced by restricted lip
GROWTH & DEVELOPMENT: As a tethered lip tissue pulls on the gums (gingiva), in due time, that point of attachment may recede. This recession can be apparent at birth or may take decades showing up in the later years. Lip restrictions may take a toll on gums, on the bone beneath the gums, or even segments of the face. Upper jaw is collectively known as the maxilla. The anterior portion of the upper jaw is known as the "pre-maxilla" which contains the upper front teeth. When the tethered upper lip pulls on the gums and jaw, sometimes we see a "harness" affect on this palatal region/upper jaw/pre-maxilla. The number of cases and arguments for this direct "harness" effect may not be so strong currently, however, the indirect effect on palatal deformation via improper suckling of the infant is more pronounced and established. Either way, the pre-maxillary sutures are usually still open at 12 years old; so, orthodontic and orthopedic treatment can remedy the situation at that age, if not earlier around 8 years of age by means of interceptive orthodontics; interceptive orthodontics usually provides jaw correction with orthopedic appliances such as palatal expanders, headgear, etc. However, the damage to periodontal tissue such as the gums or bone are a bit more delicate to repair as adults. In an infant, reversal of such early periodontal damage can be seen within weeks or months post frenectomy; whereas repairing chronic periodontal damage such as gum recession in the adult is sometimes met by many times an unsightly, very painful, sometimes unpredictable means of what is known as a gum graft. In the words of parents who discussed their personal experiences with gum recession repair: "I thought I was a tough guy, until I had a gum graft; after that I requested cadaver skin on the other areas of my mouth"; another parent stated "I did not want cadaver skin in my mouth, until my gum graft fell off...now I don't know what to do"; for her the cadaver option was a religious dilemma as well.
Palate deformation directly or indirectly by improper feeding mechanism
Additional orthodontic years interceptive/phase 1 orthopedic jaw correction
Additional orthodontic expense interceptive/phase 1 orthopedic jaw correction
Bone loss following tension forces
Gum recession following bony changes
Financial cost for periodontal surgery
Extreme pain from harvest site of gum graft
ESTHETICS: Lip ties with varying degrees of restriction place varying amounts of tension forces on the bone supporting the teeth (alveolus). Tension forces induce bone dissolving activity to rise and what some refer to as "notching" may appear.

Have you ever said to a friend: "by the way there is a piece of black pepper or something stuck in between your teeth...for a few weeks now" wondering if he flosses? I have. I feel bad about it in retrospect... as he looked down and said "no...that's just space". As the bone recedes so do the gums; and the papilla filling in cannot always keep up and the space that is left open appears as a black spot.

This black spot, regardless of the imagination of others, is just space. Since the inside of our mouth is not lit, this space looks black; a color that does not match anything else in our mouths is thereby mistaken as trapped food. With regards to esthetics, lip ties may also restrict our smile. Lip ties tie lips to gums. Whether smiling, clearing food, or kissing, a lip tied individual has a mechanical disadvantage that may translate into a functional disadvantage and possibly even an esthetic issue.
Dark spot in between front teeth
Smile unnatural lip movement
SOCIAL: Tongue ties normally get all the attention as having the potential to impact people's social lives, but one might argue that lips are important in the same regard.
Kissing restricted lip movement
TRAUMA: Extremely common are physical damage to lip ties as a result of accidental trauma. Some evidence of trauma is evident on infants as the lip tries to flange outward during suckling and minimally tears to do so; other times the evidence is far more dramatic such as when I lost my front two permanent teeth in a biking accident. Life goes on and we recover. However, suggestions by some providers that a treatment option is to allow it to tear on its own is mindless and ignorant. Such tears may be followed by a bleeding episode, a less than ideal hanging flap of tissue, and possibly an infection. Thankfully and accurately it is generally accepted that the bleeding episode is usually minimal or contained by pressure hemostasis, generally healing is of acceptable esthetics, and without infection. However to invite an accident as a form of treatment option is unacceptable. In the words of the great educator and clinician Dr. Larry Kotlow such advice by health care providers amounts to no less than "supervised negligence" which constitutes poor treatment advice and a liability. Trauma to upper lip ties are very common; bleeding can be massive depending on the accident and the mindfulness of the surrounding help; infection is possible and does happen. The worst oral infection I have ever witnessed on an infant was a 9 month old infant referred to me for multiple teeth extractions due to a very large "dental infection";

it turned out there was no dental infection but there was a massive hard tissue and soft tissue infection sequel to an accidental lip tie trauma. Also, accidents commonly leave behind a less than ideal release with obnoxious flaps of tissue in random configurations;

this new possibly unwelcome lip tie anatomy can actually make a proper release more complicated and therefore more unpleasant for the patient.
Trauma lip tie accidents are very common
Bleeding episodes may be of varying degrees
Infections are rare but serious ones do occur
Esthetics trauma leaves behind less than ideal anatomy
Harsher revision may be longer and more intricate after trauma
EASE OF CARE: A lip tie revision can be relatively convenient and comfortable with proper technique and optimal equipment. A few seconds of lip tie revision generally accounts for less than 10% of the overall post operative pain and wound care nuisance if done at the same time as the tongue revision. Instances where a laser is chosen for the revision, good surgical technique, and proper laser settings, are just as important as the type of laser used. Another important motivation for parents to revise their infants tethered oral tissues is to nullify recollection of the experience. We also find that the sooner amid infancy this procedure is performed the less complications there seem to be as a less muscular, less combative, less toothy baby offers less physical opposition allowing a safer surgery; so safe of a surgery there is no need for sedation.
Minimal Memory recollection is minimized with infancy
Minimal Discomfort numbing and pain medication can be provided
Minimal Risk as infants pose a less physical barrier than young children
No Sedation needed as infants are easier to manage in a safe environment
ACCESS TO CARE: My office routinely receives requests from parents of two to five year olds seeking frenectomy service to relieve the symptoms of their children. At this time I do not treat this age group. I do respect those clinicians who are able to meet this demand but they are few and far; therefore access to competent quality care for the young child is very sparse to practically non-existent at this time. This is certainly a valid reason why some parents choose to treat their baby sooner than later; aware that many functional issues possible with lip ties may not arise, but the problems that do manifest over time may be harder to treat in childhood, quite distressful during the teenage years, and rare during the college years when time and finances seem to run thin for most in their 20's. Most clients preferring a lip tie revision for their infants find the service affordable or perhaps covered by insurance.
Minimal Financial Cost many find the fee affordable or covered by insurance
Access to care maybe higher for infants than 2-5 year olds or even toddlers
During a child's infancy parents have the opportunity to treat the functional issues risen from tethered oral tissues as well as exercising their parental right to help prevent other issues that may arise. We are an active partner in the parents informed decision making process, but ultimately the choice is theirs to make. We have chosen to be supportive of people’s right to treat current problems, the right to prevent future problems, the right to wait and observe, as well as the right to continue learning and amass the knowledge needed to feel at ease with their decision.
Dr. Shervin Yazdi, DDS
Copyright 2020 All Rights Reserved






Comments